
Avoiding the Gerontocene
America’s choices on policy and research priorities today could determine whether the coming decade brings us yet closer to a shrinking fraction of healthy Americans attempting to support the aged.



America’s Scientific Ascendancy
In November of 1944, President Franklin D. Roosevelt wrote a famous letter to Vannevar Bush, director of the Office of Scientific Research and Development. Roosevelt asked him how America’s scientific prowess would guide the world and benefit the public in the post-war world.

Vannevar Bush (Credit: H. WALKER/TIME LIFE PICTURES/GETTY)
Bush’s response was a report detailing “The Endless Frontier” of American innovation, fueled by public investments in scientific research, strong relationships with academic institutions, and resounding support for the early research that would go on to enable countless cures, energy improvements, material development efforts, and even put a man on the moon. This system has driven incredible biotechnology research, leading to improvements in our span of healthy years. The results have ranged from better hygiene to novel therapies for cancer and neurodegenerative diseases.
However, an end to the Endless Frontier is now on the horizon.
The Choice Ahead
As the American population grows older, the economic and personal burden of age-related disease grows more stark, straining Medicare, Medicaid, and other social welfare systems. This is compounded by age-associated ailments taking away late-life productivity. It’s time to revisit the question of how America’s scientific prowess will benefit the public. The original Endless Frontier began at a time when the biology of aging wasn’t a topic of research, and efforts to combat disease were divided on many fronts rather than studying their shared causes. As our understanding of aging biology evolved, this framework did not, and today still only ~1% of the NIH budget is directed towards addressing the largest risk factor for most diseases: aging. Targeting one disease at a time, sometimes referred to as “sickcare”, is seeing diminishing marginal returns in aging populations, as each new medicine offers a short-lived reprieve from disability. Addressing the root causes of aging, on the other hand, could lead to accelerating improvements in health and quality of life. Yet, ongoing cuts to basic scientific research are hindering our ability to understand — and intervene in — these aging processes. Strategic investment is also drying up as biopharma increasingly taps late-stage assets based on past research and relies on Chinese innovation, presaging a future where Americans are sicker for longer. Meanwhile, other countries, such as China and Singapore, are investing heavily in their domestic ability to both innovate and manufacture new interventions for chronic and age-related diseases.
Nations must choose whether to lean into the biology of aging for solutions to public health or stay reactive to a growing burden of disease. Eighty years after initiating The Endless Frontier, America is faced with this choice as well as the consequences it will bring. On one path, our ignorance of aging biology leaves us helpless to prevent the financial, emotional, and physical consequences of an aging population. On another, we ensure that every American can live healthier for longer, free from mounting pill bottles, medical debt, and chronic suffering.
Let’s explore what each of these futures might look like…
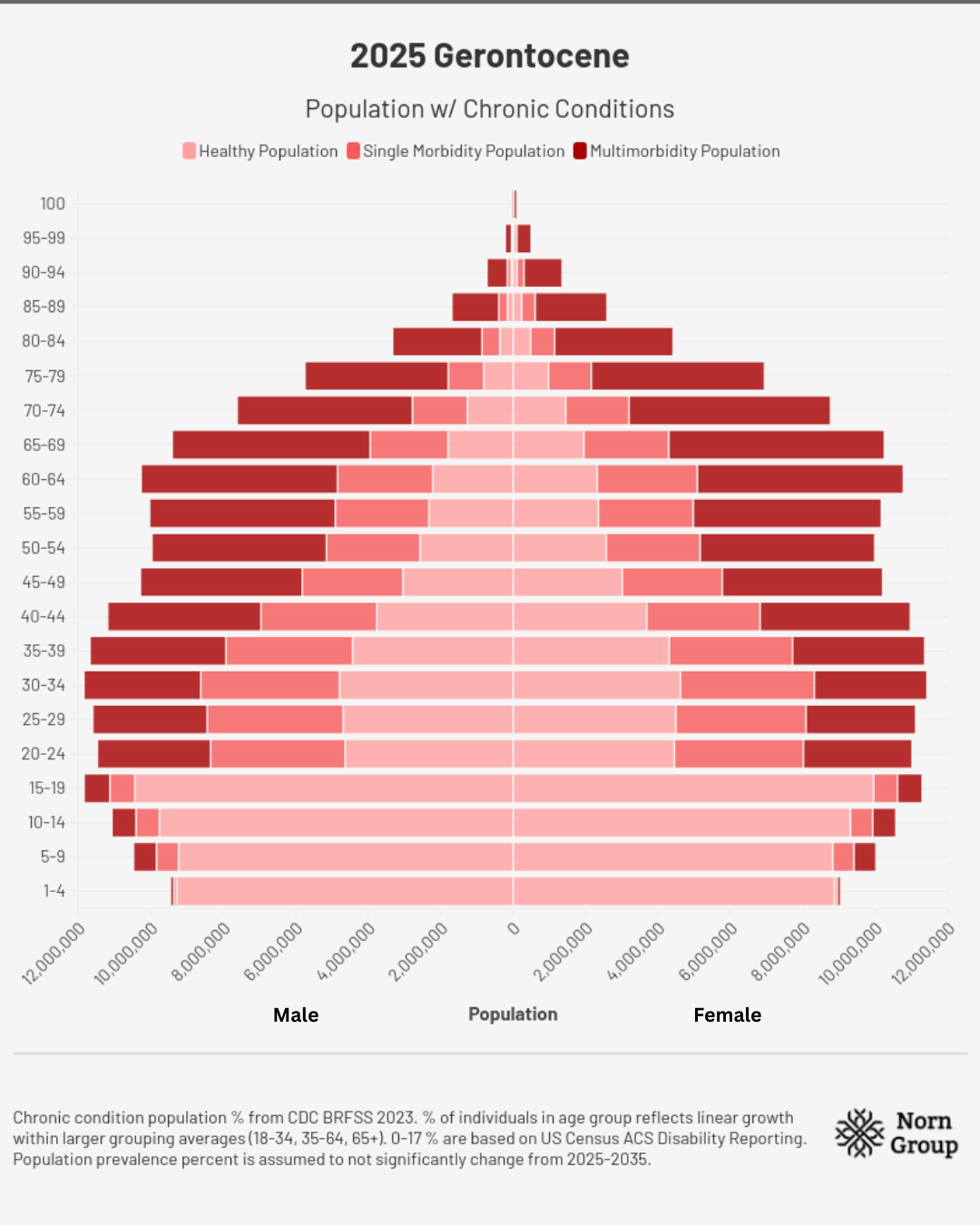
The Gerontocene
2025 | A Missed Opportunity
Under the shadow of ongoing debt negotiations, major spending bills, and other budgetary constraints, debates erupt in the U.S. Congress over healthcare and research spending. The rising number of older Americans relying on Medicare/Medicaid and Social Security spurs belt-tightening efforts that slash discretionary spending and grant programs. On top of research funding cuts, increased uncertainty about future drug approvals causes investors to pull capital from early-stage innovation. Pipelines shutter and many smaller companies close their doors, firms are increasingly competing for the smaller pool of later-stage assets within the American and EU markets, and are increasingly turning to Chinese offerings. As institutions slash budgets to account for reduced federal funding, young investigators are lured eastward and to Europe, as both spheres of influence compete to attract talent fleeing U.S. institutions. These consecutive hits deal a lasting blow to the biotechnology industry and the development of therapeutics for diseases of aging.
In the midst of all of this, the rise of GLP-1s after two decades of effort gives the industry a lifeline: a strong and very profitable example of one drug addressing multiple diseases. Experts across the nation spotlight the widespread applicability and apparent safety of GLP-1s – some hailing them as the “first longevity drugs” – emphasizing the broad economic implications of a society less riddled with obesity, diabetes, and other conditions. However, this success depends heavily on decades of prior research. Some scientists view aging biology as a field with the potential to yield the next such drugs. But public fears and doubts from other doctors and scientists scare off politicians from supporting this new approach. Rather than doubling down, the U.S. shies away, with budget deliberations upholding reductions to NIH funding for aging projects and regulatory proposals being ignored.
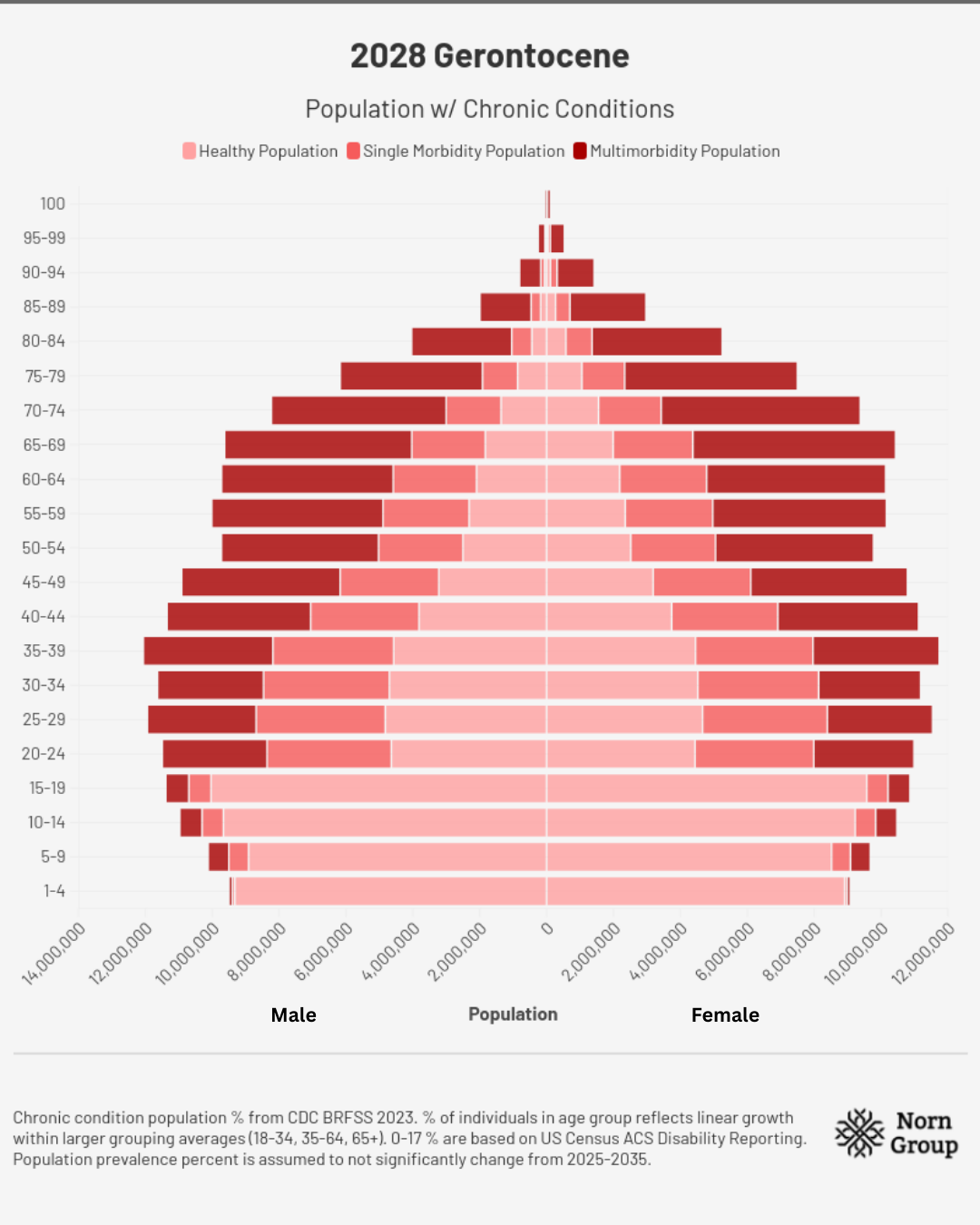
2028 | Warning Signs
Healthcare disparities make headlines throughout the country: Nearly 70 million people in the US are over the age of 65, and ~80% have two or more chronic diseases, requiring multiple daily medications. As the incidence of age-related disease rises, insurance premiums continue to climb, leaving many middle- and lower-class families to forgo medicines. The situation strains hospital and provider networks while also pushing long-term care infrastructure to its limits. Shortages of professional caretakers, cuts to at-home care eligibility on Medicaid, and subsequently long wait lists all contribute to worsening healthcare standards. The human toll falls on the 70 million Americans who serve as unpaid caregivers, left with little choice but to reduce their working hours or take career breaks entirely to provide for loved ones.
Medicare spending passes $1.5 trillion this year. Politicians are at a loss for options to address the crisis, short of making further cuts or facing tradeoffs with other expenses such as defense, education, and infrastructure. Social Security barrels on track towards insolvency by 2033, and more cuts are made to key services for seniors and retirement benefits. While this plays out, China announces several national moonshot programs intended to target aging and chronic disease, some of which are led by U.S. scientists who left the country following budget cuts in 2025. Investors and innovators alike continue to shift eastward, pouring a growing amount of capital into deals with Chinese companies. This shift drains the American biotechnology sector of cash flow for new startups and scientific spinouts.
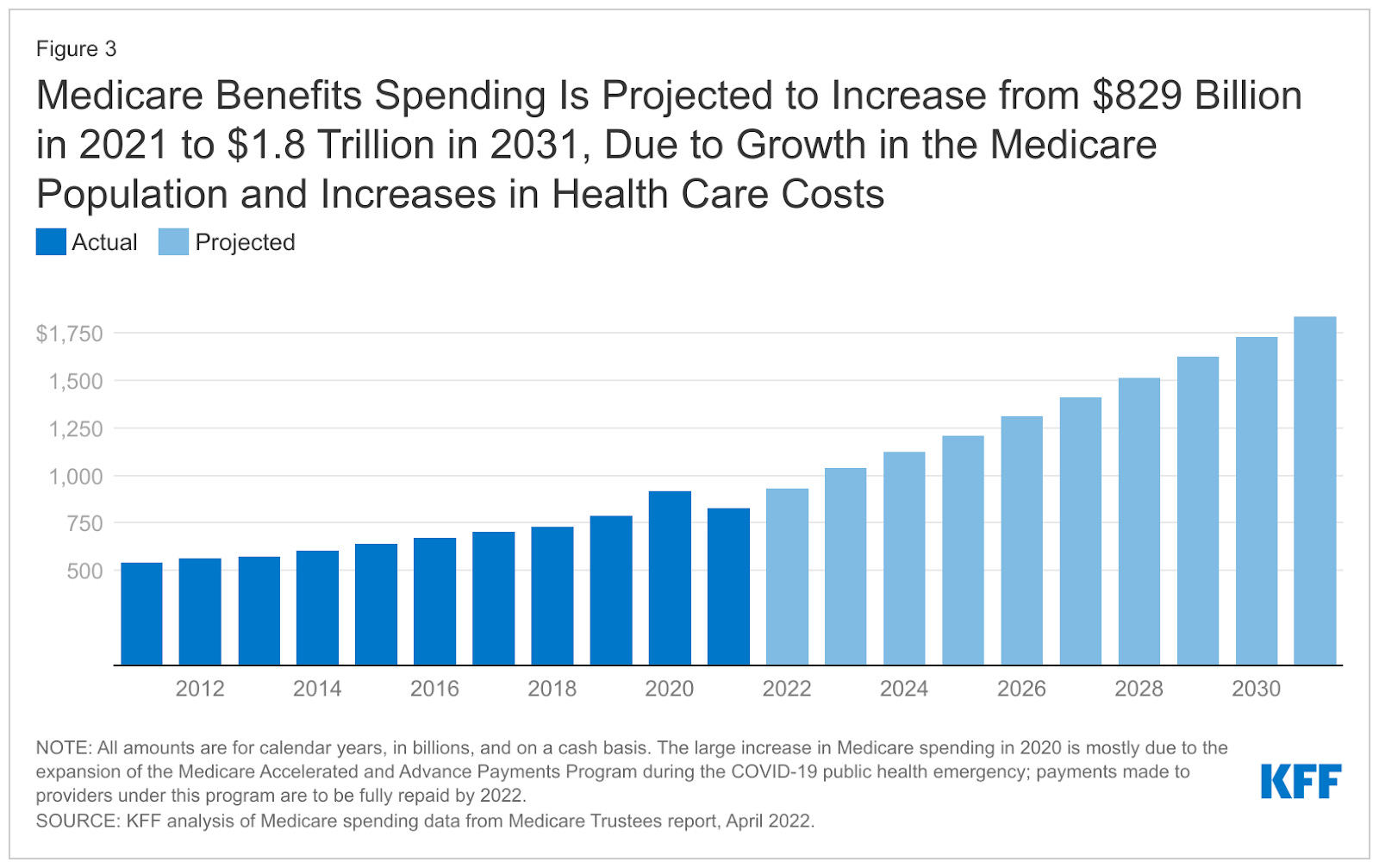
Source: KFF
With all these factors, the engine driving us into The Endless Frontier begins to stutter. Universities report drastically lower numbers of matriculating graduate students, and investors lament over the shriveling early-stage pipeline of new medicines. Much of the scientific community realizes that if action is not taken soon, there will be no reversing the collapse.
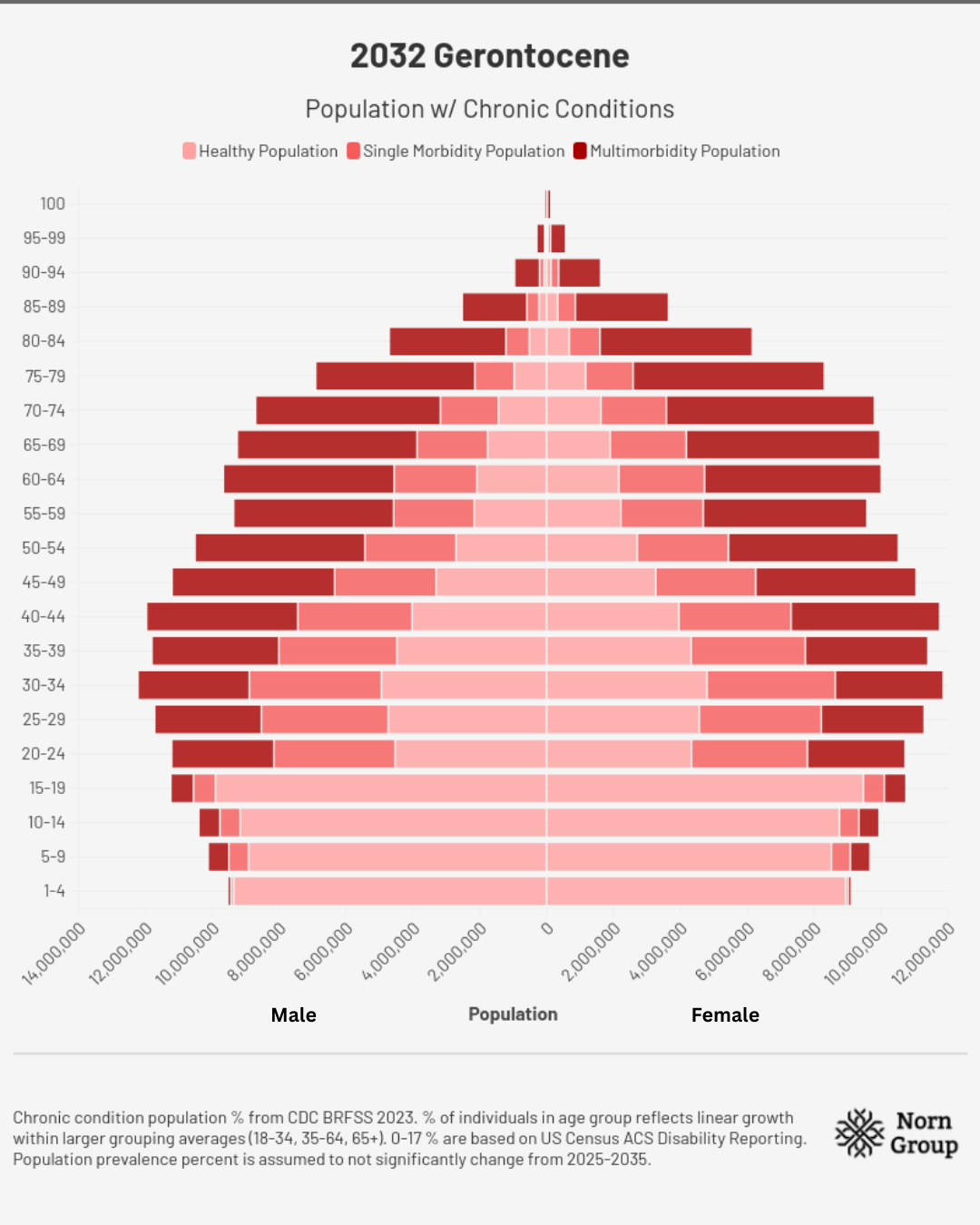
2032 | Turning Point
As the nation rings in the New Year, the Bureau of Labor Statistics reports that a record number of individuals left their jobs to care for an older loved one. The special report shows Americans citing unbearably high costs, years-long waitlists, or a lack of a care facility within distance as the main prohibitors. Adding to the expense is the fact that many are still being treated for individual diseases on a reactive basis. As the number and prevalence of these diseases increases, the personal and societal costs grow, putting treatment out of reach for many patients.
Sharp restrictions on Social Security eligibility are put in place by Congress as the program’s ability to make payouts reaches a crisis point. Meanwhile, more stringent working requirements for Medicare and Medicaid are enacted, putting further financial strain on families to afford care. Workforce participation sinks among Americans over 65 for the first time since the pandemic due to the rising number of Americans living longer, but being unable to work due to age-related diseases. Shortages across sectors, including healthcare, education, and the trades, draw comparison to Japan’s trends in the previous two decades. With an old-age dependency ratio of 35% and a total of 72% (i.e. for every 28 working individuals, there are 35 dependent seniors), proposals are circulated throughout the U.S. Congress to raise the retirement age in order to keep Social Security afloat.
Across the Pacific, China’s state-sponsored longevity efforts have begun to pay off, so far resulting in the first aging therapeutic targeting multiple indications and increasing healthy life at a lower cost. However, due to ongoing geopolitical tensions, U.S. access to the drug is limited. With a diminished biotechnology sector and growing reliance on Chinese organizations for biomanufacturing, efforts to produce a similar therapeutic will take years. In the meantime, Americans are left to forgo the benefits. Chinese citizens, however, enjoy a reduced disease burden and less dependence on care or prescriptions. Leaders note marked reductions in hospital admissions for age-related diseases and fragility, while families enjoy the reduced pressures of caretaking responsibilities. All of this is possible despite nearly two decades of a challenging demographic picture resulting from the one-child policy.
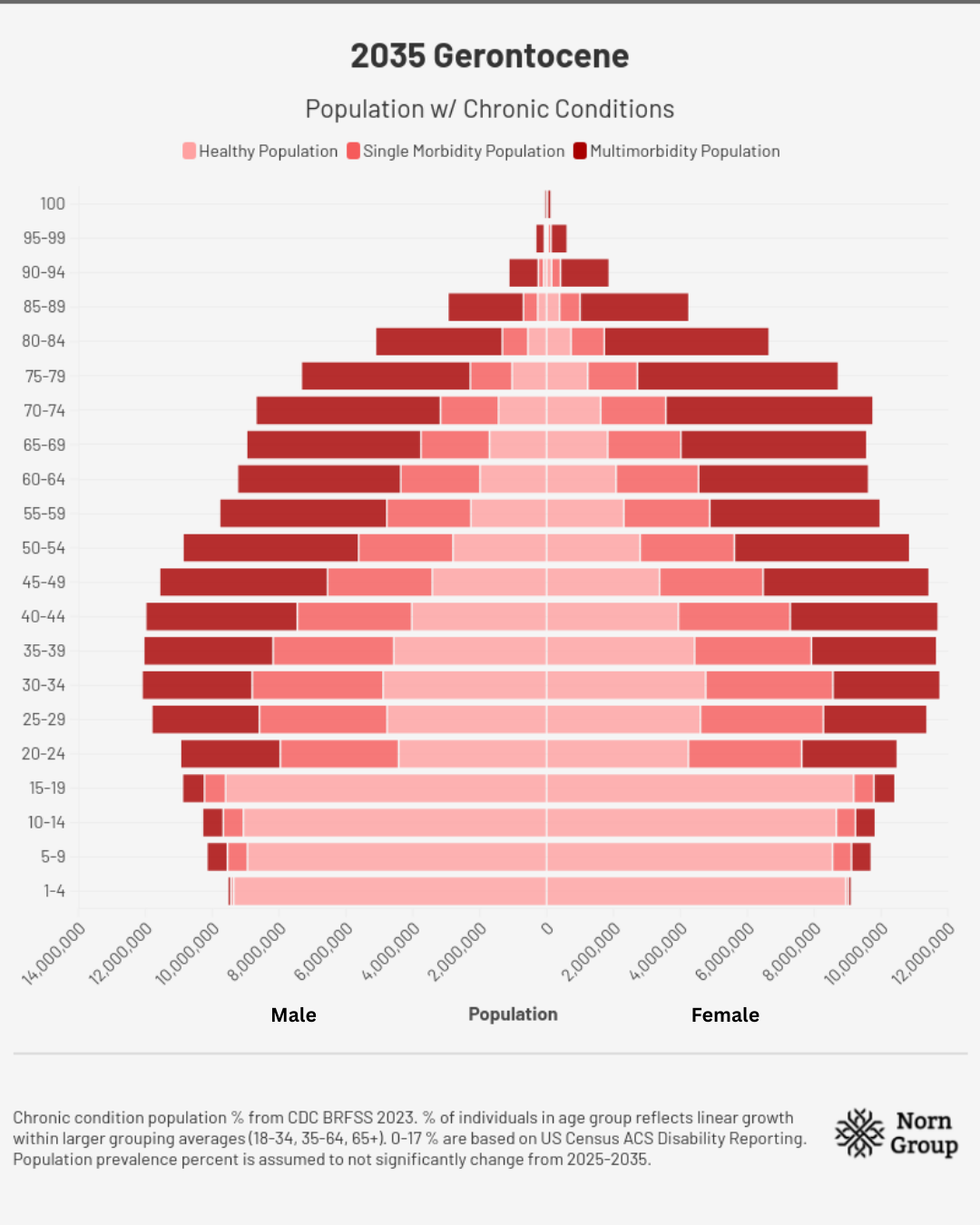
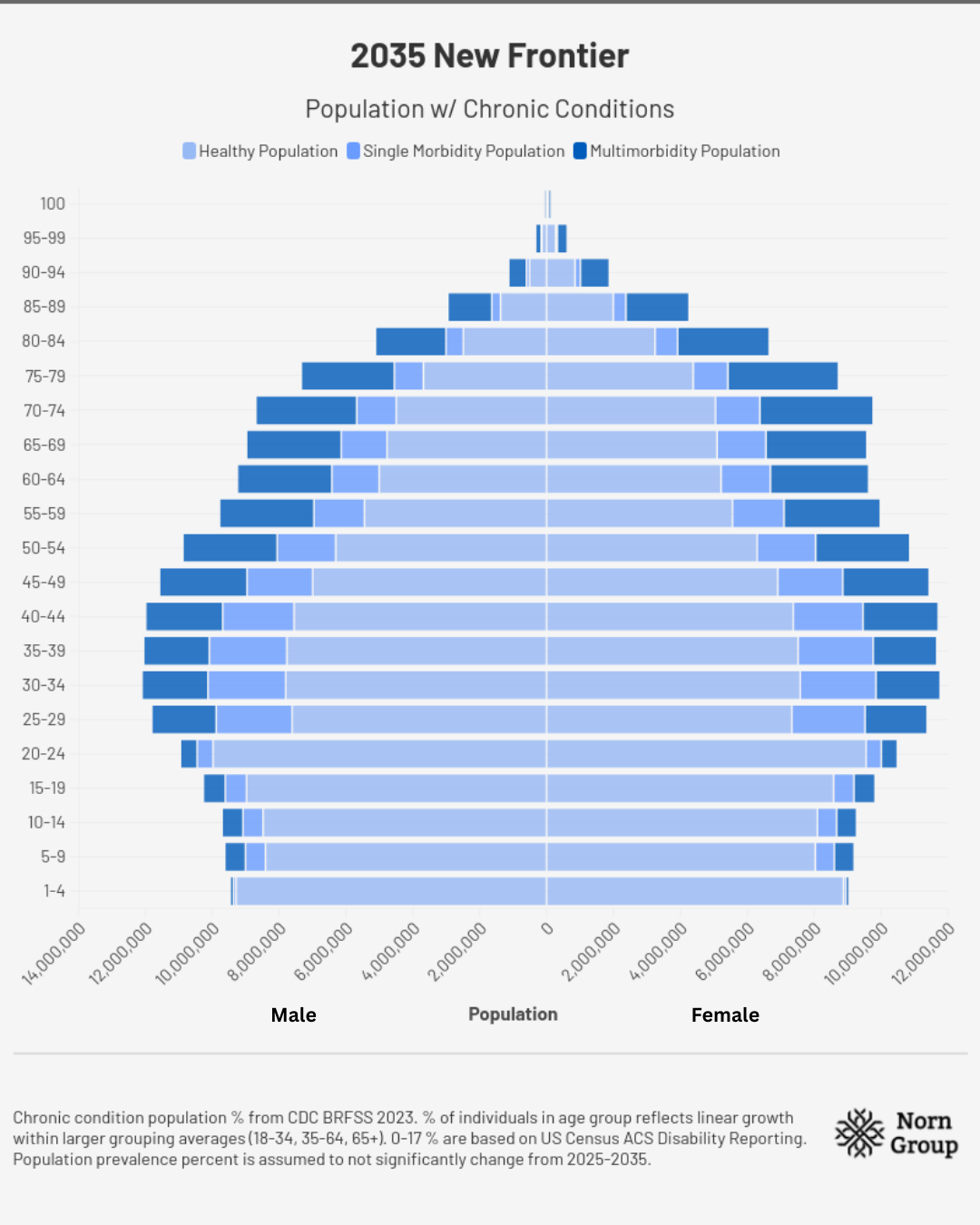
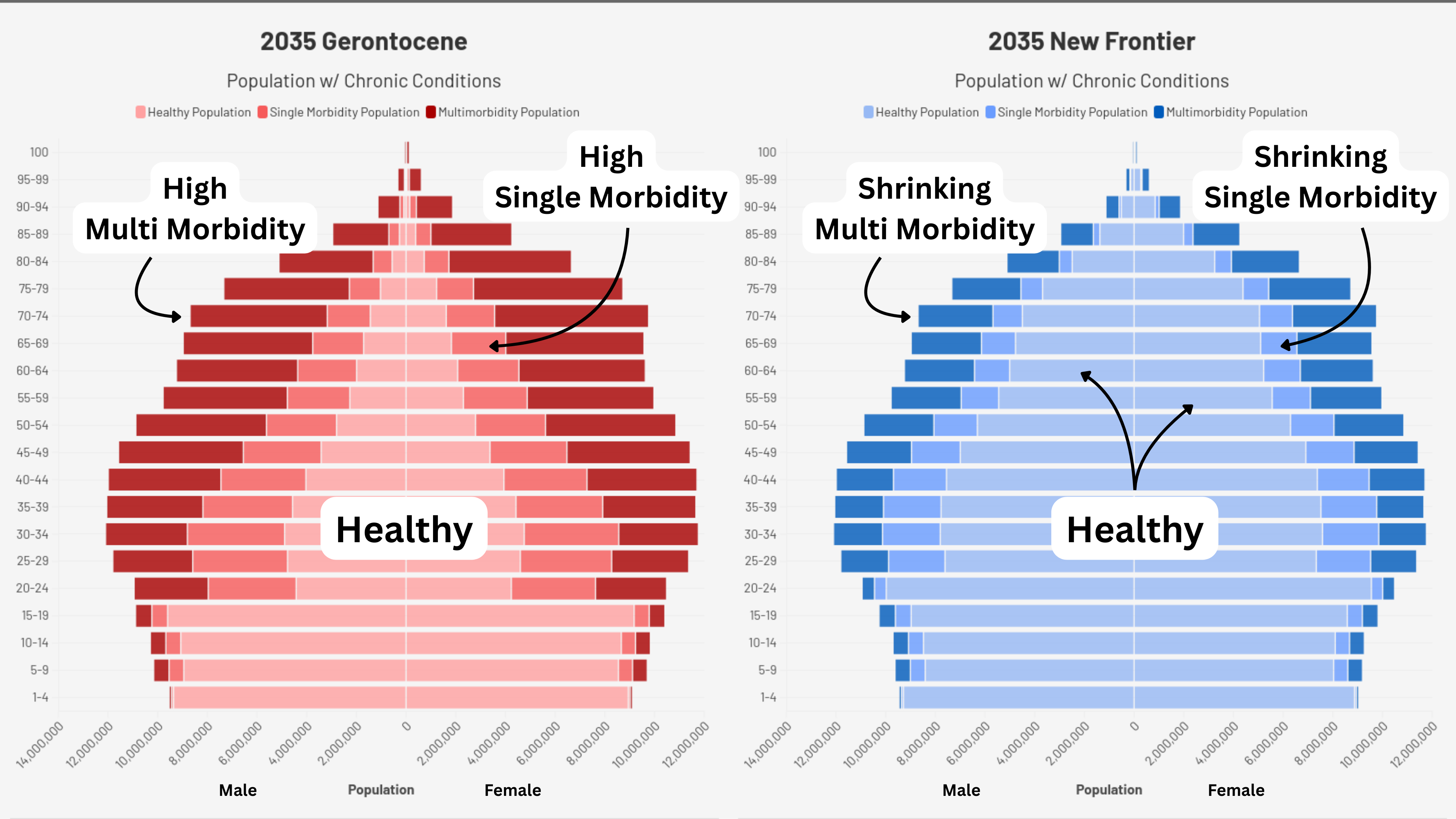
2035 | The Gerontocene
For the first time in American history, falling fertility rates have led to the number of individuals over 65 outnumbering those under 18. A decade of insufficient investment in aging therapeutics has produced the “Gerontocene” – a world where social structures, economics, and happiness are dominated by the ills of aging and our inability to combat them.
Successful development of aging therapeutics overseas from adversarial nations has created stark contrasts in quality of life and economic output. However, geopolitical tensions continue to prevent Americans from broadly accessing them. After seeing the possibility demonstrated abroad, American politicians and regulators reverse course, announcing a moonshot program investing billions of dollars into the development of a comparable multi-morbidity therapeutic. Big pharmaceutical companies and startups alike begin spinning up programs to answer the call. However, official predictions do not anticipate the completion of the program or widespread availability to the public for at least another 10 years – a decade of decline under the shadow of the Gerontocene.
How can we avoid this fate? Let’s take a look at another path, of boldness and hope.
2035: The New Endless Frontier
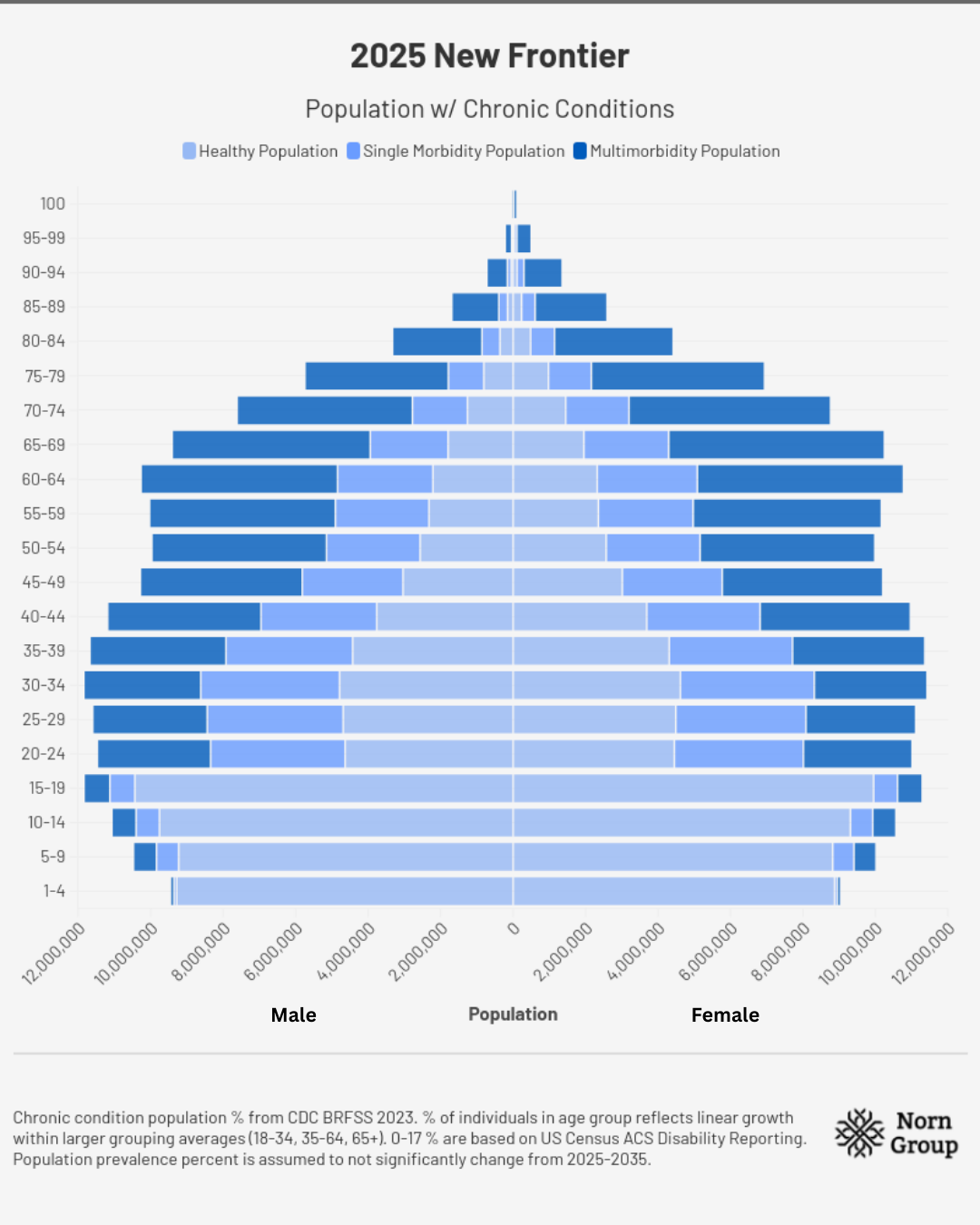
2025 | The Beginning
The Secretary of HHS spends his first months in office focusing heavily on the prevalence of chronic disease, stating, “The chronic disease epidemic is the most urgent and costly health crisis in America today. We can’t afford another decade of delay.” Prioritization of chronic disease at the highest levels of government leads to investment and research into shared causes of many diseases. This momentum leads to several executive orders being signed to support aging therapeutic innovation. These orders build on the progress of several ARPA-H programs launched earlier in the year to target age-related conditions and upstream causes of aging. Simultaneously, the White House announces the creation of a public-private investment partnership, similar to those seen with AI innovation. Leaders see it as an opportunity to capitalize on the enthusiasm from recent blockbusters such as GLP-1s, the expanding market size in an aging population, and rapidly maturing science in the aging field.
China, recognizing the demographic crisis in its own rapidly aging population, follows America’s leadership in this space and begins to accelerate. Expanding its Healthy China 2030 agenda, China invests heavily in aging therapeutics to counter American development and sets its eyes on higher life expectancy goals. However, thanks to moonshot programs such as ARPA-H and strong public-private interest, the U.S. takes the lead, attracting more talent, investment, and popular support than our competitors. The New Endless Frontier is on the horizon, and just as we did with the race to the moon, we are not shying away from the moment; we are bringing the future to fruition.
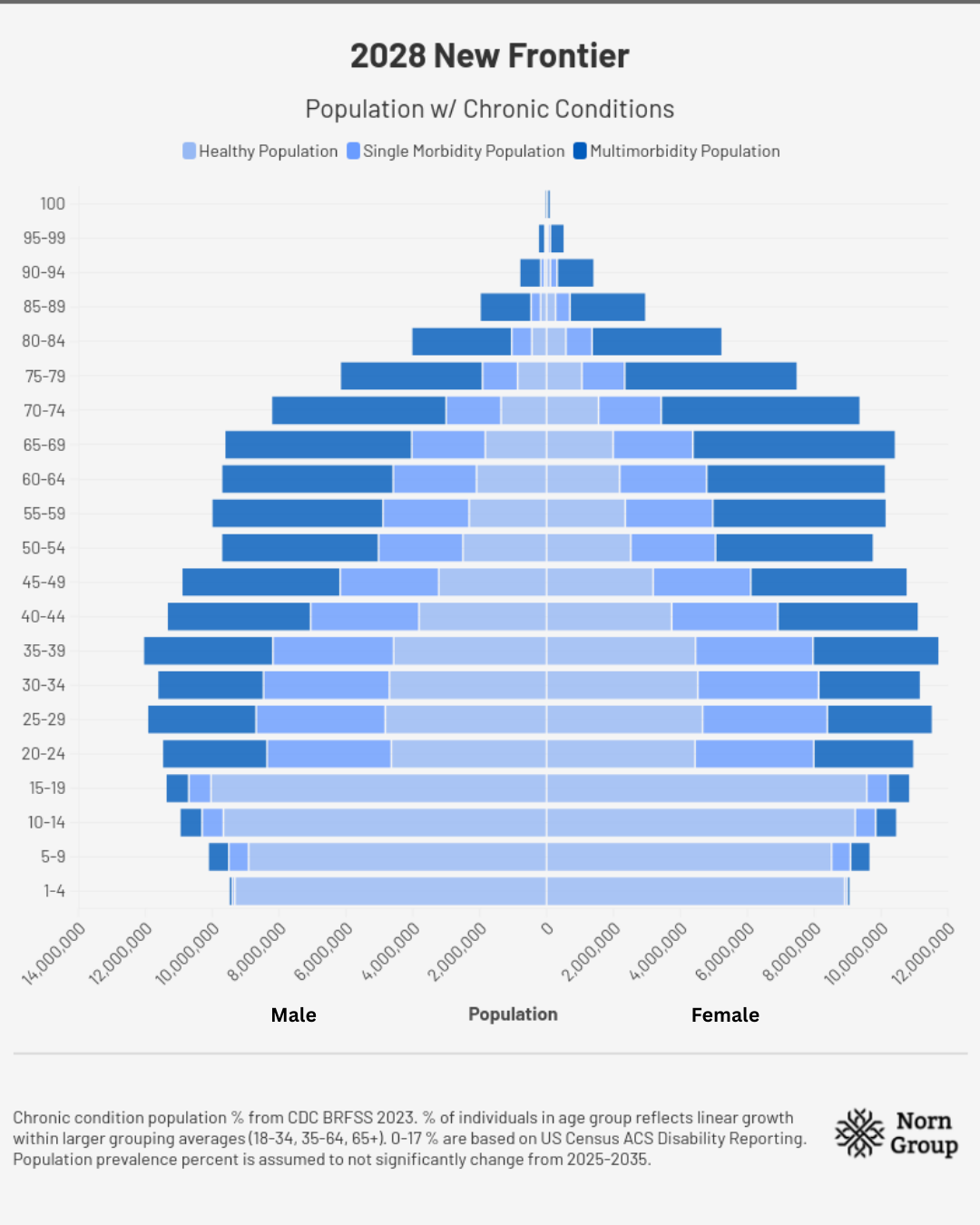
2028 | A Rising Tide
By 2028, following intense efforts to reform regulatory consideration of aging therapeutics, the first clinical trials for “aging indications" are launched under advanced conditional approval pathways. The earliest Phase 1/2 trials are of existing medications that were previously only approved for single indications. The announcement spurs excitement, generating a wave of investment into new and existing companies to develop drugs specifically for aging. By this point, billions of dollars have been poured into combating age-related diseases. Hundreds of preclinical studies are conducted, innovating on new drugs, attempting to repurpose new ones, and developing novel biologics. Growing understanding of aging processes and their manifestations underlie this upswing in the space.
A new wave of venture capital firms focused on longevity pop up, building on the success of the pioneers in the field. With this momentum, Congress raises the NIH’s investment in aging biology research for the third consecutive year, with FY29 levels double what they were in 2025. American biobanks, such as the All of Us program, continue to unlock troves of data about healthy and super agers, attempting to crack the genetic, environmental, and behavioral code of living healthier, for longer.
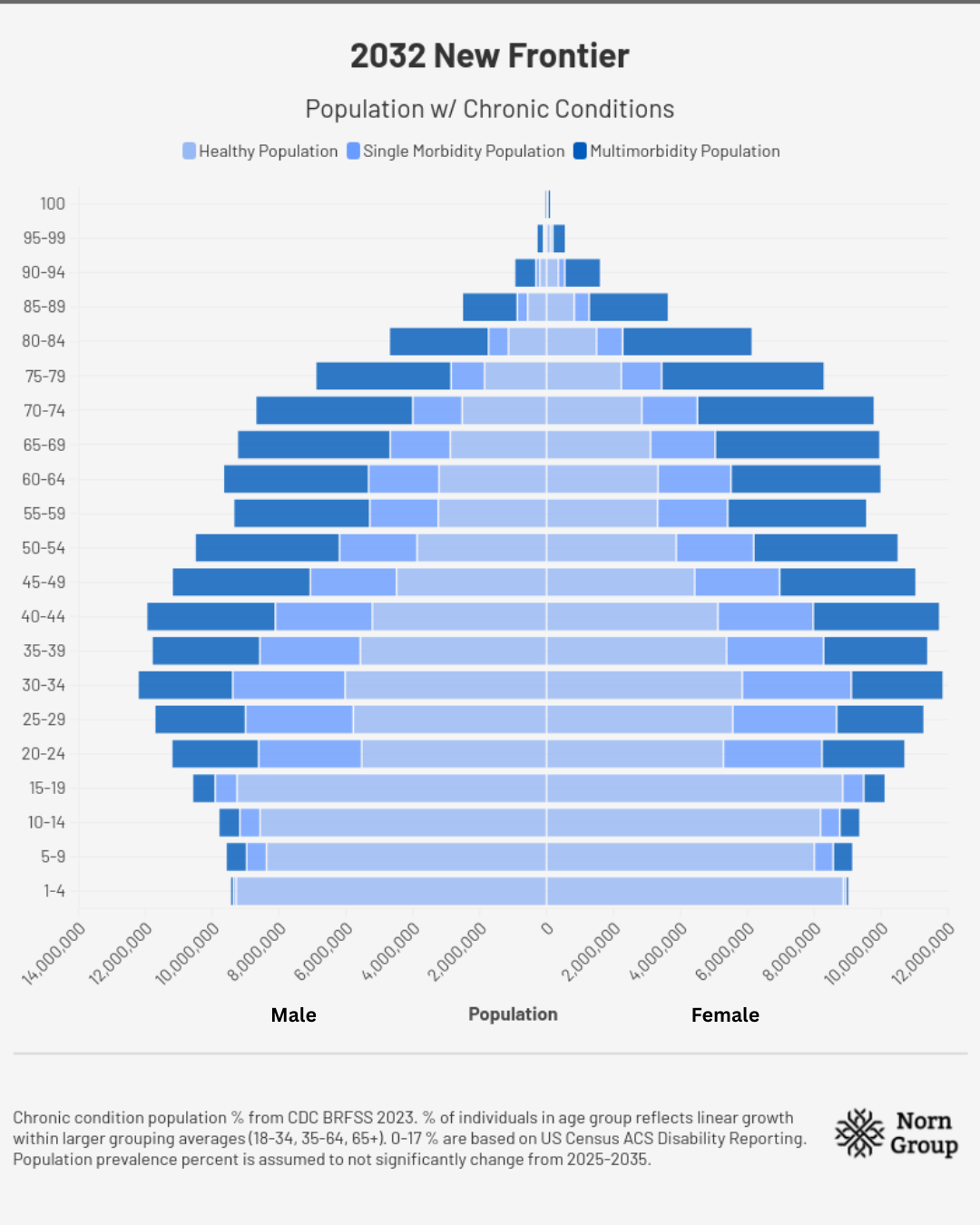
2032 | Breakthrough
In 2032, the first aging therapeutic is approved in the United States based on broad benefits across disabilities. A drug that was previously approved for a single indication is now widely available to tens of millions of Americans. After showing a 30% reduction in frailty and significantly improved cognition in a placebo-controlled phase 3 trial, FDA advisory boards are quick to recommend the approval of the drug under the new “aging indication” pathway created in 2028. This marks a milestone in humanity’s progression towards improving our health and beating back the diseases that have plagued our species since its inception. The drug is linked to a reduced risk of cardiovascular and neurodegenerative issues, enhanced physical stamina, and better cognitive capabilities to heightened workforce participation. By the end of the year, the percentage of the population over 55 participating in the workforce crosses 45%, thanks largely to lower disease incidence.
Within just a few years, the economic returns start to be felt, with some Americans reporting fewer hours spent caretaking for older loved ones and lower medical debt as a result of fewer falls, diagnoses, and medications needed. As the availability of these drugs spread, there is a noticeable decline in Medicare and Medicaid claims, despite a growing number of eligible individuals. Realignments in retirement plans seek to provide flexibility to older workers who are gainfully employed, not because they have to, but because they want to and can be. Around the country, waitlists for long-term care facilities drop, while hospitals see declines in the number of visits for age-related diseases and frailty-dependent falls among older individuals.
This trend is especially true in areas of the country where adoption of these drugs is high. Congress, looking forward to the FY33 budget, sees stabilization of Medicare and Medicaid costs, freeing up the opportunity to pursue payments on debt, investment in infrastructure, and other key discretionary topics. American cities retain the lead in investment and talent attraction compared to other global hubs.
2035 | The New Endless Frontier
By 2035, Americans start to benefit from a system that truly focuses on healthcare, rather than reactive “sick-care”. Years of public funding to understand basic aging biology have created a rich pipeline for continued development of drugs that more efficiently reduce disease burden. 2025 served as a crucial moment when many other nations were seeking to dethrone our leadership in science. Strategic competitors sought to become home to the latest revolution in human health through the development of aging therapeutics. However, the U.S. government rose to the occasion, creating the conditions (regulatory and otherwise) for a whole new class of “longevity drugs” that became first available to the American public.
On the back of strong public-private partnerships, an influx of investment for the space was curated. As the field continues to expand, people worldwide rely less on different drugs to manage multiple chronic diseases and instead take one to combat many if not all. With their strong safety profiles, these drugs are prescribed preventatively for individuals almost as commonly as statins were for cardiovascular risk just 10 years ago. Close attention from the FDA to the value of quality control reduces “snake oil” offerings and uplifts credible interventions. The U.S., partnering with dozens of allied nations, leads a global initiative committed to distributing aging therapeutics, setting the moral, scientific, and economic momentum to tackle chronic diseases.
Expectations of financial ruin from Social Security insolvency never materialize. As a result of fewer Americans needing expensive long-term health care or costly prescriptions, average individual beneficiary claims continue to shrink. Many adults who otherwise would have had to take breaks in their careers to care for aging loved ones or incur crushing medical debt can instead enjoy more time with those in their lives. The economic boost and reduced societal burden of age-related disease secure America’s role as the global leader on health, freeing up investment into other discretionary areas of spending.
A New Endless Frontier has arrived, freeing humanity from the once seemingly inevitable decline that came with aging and the trap we could have fallen into where more years did not mean more health, but more suffering.
Conclusions
Countless matters cry out for our attention. As a nation, we are always forced to choose our battles, and sometimes come to regret our choices. For example, America neglected to invest in industrial semiconductor chip production beginning in the 1960s. Decades of deprioritization and reliance on other nations’ capacity have led to supply chain choke points that are more vulnerable than ever to geopolitical tensions. Starting to reverse course cost ~$280 billion in the form of the CHIPS and Science Act. The same story has played out for mining rare earth minerals and conducting heavy manufacturing. As fertility rates decline, population aging continues, and treating disease becomes more and more costly, it is clear that the battle for healthy aging cannot be ignored.
What we choose to do today defines the next decade, as either an inexorable shrinking of our healthy population or the turning point towards health. Our ancestors looked to the stars, yearning to be among them. It was the United States of America that made it happen. Our ancestors have also looked to their loved ones, yearning to free them from disease and disability. Should the people of the United States of America be the ones to make it happen? If so, the choice we face today is clear.
Comments on our assumptions
Note on Charts/Figures: Charts and key numbers in this piece are not intended to be a precise analysis of how longevity therapeutics will impact economic and demographic outcomes, which would require proprietary knowledge and extensive modeling. Rather they represent what we think are reasonable estimates (more below), and leave greater precision to economists and other writers. As more information becomes publicly available, we may update this piece with new findings and models that rigorously quantify the transformational impact of longevity therapeutics.
Assumptions for demographic charts: Total populations in each age range are from the U.S. Census Bureau’s International Database. Chronic condition population percentages come from CDC BRFSS 2023. The percent of individuals in each age group reflects linear growth within larger grouping averages for disease burden prevalence percentages (18-34, 35-64, 65+). Numbers for 0-17 are based on US Census ACS Disability Reporting, as no chronic disease data were available. Population prevalence percent is assumed not to change meaningfully from 2025-2035.
Assumptions for impact of new therapeutics: We assume that the percent prevalence of disease is the same for both tracks until 2032 (for example, if multiple chronic condition burden for 65+ is reported by BRFSS is 78%, it is assumed to be 78% in both the Gerontocene and the New Frontier). For the reduction of disease burden starting in the 2032 entry, we assume a 15% reduction in chronic disease prevalence and then a 30% reduction in 2035. These estimates are based on one, then two, medicines from aging research with effects comparable to existing GLP1 agonists (such as Ozempic), roughly 20% on multiple prevalent diseases. We do not attempt to model specific efficacy on individual conditions. These reduction figures do not factor in any form of adoption percentage, discount rate, or other distribution metric.
 | A guest post by
|
 | A guest post by
|